
- NICE rejected Enhertu® for HER2-low breast cancer in 2024 – the first breast cancer treatment not recommended by the drug regulatory body in 6 years. This is not because the treatment doesn’t work, but because it costs more per quality-adjusted life year (QALY) than the NHS can afford.
- Rejected drugs can sometimes become accessible via private pathways or postcode-dependent NHS decisions, creating an unfair system where income and residence dictate access to life-extending treatments.
- A 2025 NICE threshold increase to £25K – £35K per QALY will allow more cancer drugs to be approved, but won’t address the reallocation of budgets where every additional pound spent on newly approved cancer drugs, is a pound less spend elsewhere.
How do NICE decisions work?
The National Institute for Health and Care excellence serves the primary purpose of health technology assessment (HTA). This is achieved in two ways: by providing clinical guidelines on the most appropriate treatments and care regimes and to provide guidance of whether recommended treatments are cost-effective for commission in the NHS. As of late 2025, NICE currently approves approximately 91% of the medicines it evaluates; around 70 per year. The 9% that are rejected often represent significant unmet clinical needs, creating the tension between cost-effectiveness and patient access.
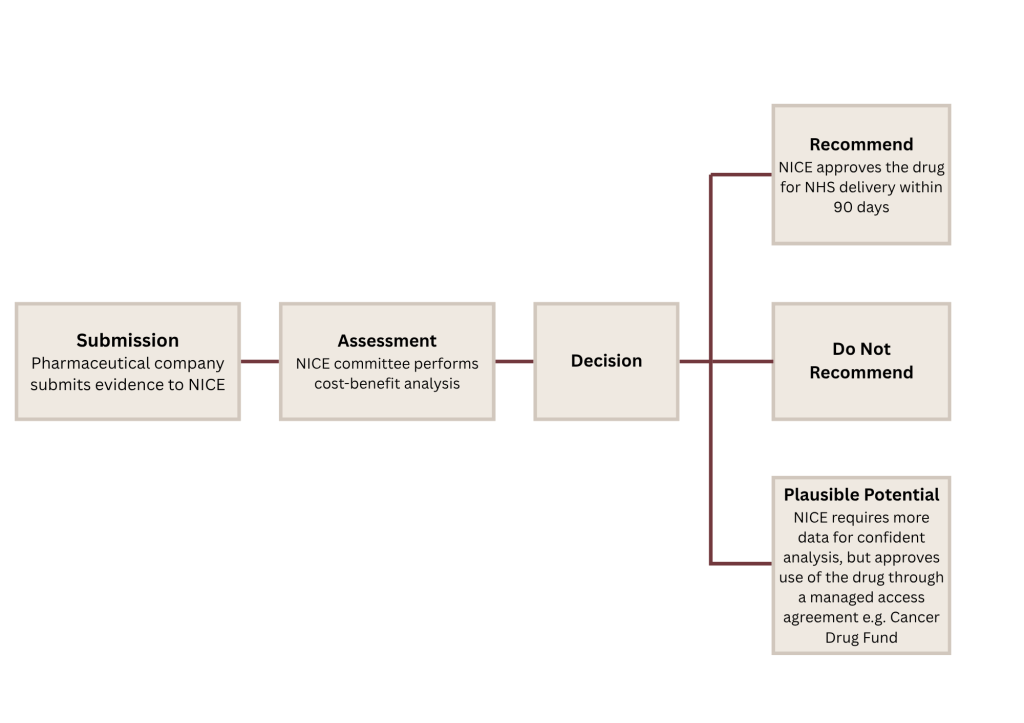
The decision making is a multi-step process involving the pharmaceutical company producing the therapy and a panel of experts. NICE uses the clinical trial evidence provided and performs their cost-benefit analysis to make their decision. From April 2026, NICE will approve new therapies if they provide an additional year of good health for between £25K to £35K. However there are also instances where NICE do not provide guidance and instead reject commission in the NHS.
How NICE measures cost-effectiveness
QALY (Quality-Adjusted Life Year): A measure that combines the length of life with quality of life. One year in perfect health = 1 QALY. One year with significant health limitations may = 0.5 QALY.
ICER (Incremental Cost-Effectiveness Ratio): The additional cost per additional QALY gained compared to current standard treatment.
Example NICE assessment: A new cancer drug costs £40,000 per year and extends life by 6 months in good health (0.5 QALY), compared to a standard treatment costing £10,000:
ICER = (£40,000 – £10,000) / 0.5 = £60,000 per QALY
NICE decision: At £60,000, this drug would be rejected unless severity modifiers apply.
Cancer drugs are particularly affected by NICE’s cost-effectiveness framework as they often deliver modest life extension at a very high cost, exceeding standard thresholds. Unlike preventative treatments or early stage interventions, late-stage cancer therapies address urgent, life threatening disease making rejections extremely difficult for patients and clinicians. NICE has recommended or given a plausible potential decision on 81% of the cancer drugs they have assessed.
What happens when drugs are rejected?
You’re probably wondering why a drug would be rejected? If evidence supports the improved quality and length of life, it should be available on the NHS without any questions asked. Well, other than the cost-benefit analysis there are other factors which may lead to NICE being unable to provide guidance and approval. Below are a few real world examples of rejected cancer treatments.
Case study 1: Enhertu® for advanced HER2-low breast cancer.
Enhertu® (Daiichi-Sankyo and AstraZeneca) is an antibody-drug conjugate designed to target cancer cells expressing the HER2 receptor. Studies have demonstrated improved progression-free survival and extension of life with Enhertu®. It is FDA-approved in the USA for multiple indications of HER2-positive and HER2-low breast, lung and gastric cancers. In Scotland it is SMC (Scotland’s equivalent of NICE) approved as a monotherapy for HER2-positive breast cancer where previous targeted therapy has failed.
In 2024 NICE could not provide guidance on Enhertu® and rejected the therapy due to an unfavourable cost-benefit analysis. NICE claimed whilst they and the NHS offered cost flexibility, Daiichi-Sankyo and AstraZeneca did not offer an improved price. However, guidance is still under review, and the threshold changes may reverse the current decision. At least 55% of all breast cancers are classified as HER2-low.
This cost-effectiveness-based rejection highlights a core tension of NICE assessments; the drug works, but at a cost beyond what the NHS budget allows. The question is not whether Enhertu® can improve quality or length of life but whether £X per year of life with Enhertu® is a responsible use of constrained NHS funds, especially when the money could be applied in other areas like screening programmes or social care.
Case study 2: Elahere for folate-receptor positive platinum-resistant advanced high-grade serous ovarian, fallopian tube and peritoneal cancers.
Elahere (Abbvie) is an antibody-drug conjugate designed to target cancer cells expressing Folate receptor alpha. Multiple studies have demonstrated improved progression-free survival, overall survival and improved objective response to chemotherapy. Elahere is FDA and SMC approved, for folate-receptor positive platinum-resistant advanced high-grade serous ovarian, fallopian tube and peritoneal cancers.
In 2025, NICE were unable to provide guidance on Elahere due to low cost-benefits and uncertainties surrounding: 1) How life differs for people using Elahere vs traditional chemotherapy, 2) How long people live after Elahere treatment, and 3) The average age of those starting the treatment. When NICE considered the disease severity and effect on quality of life, the cost-effectiveness estimates were out of range and not acceptable for the use of NHS resources – however this is still under review. Approximately 80% of recurring ovarian cancers present with Folate receptor alpha with up to 36% classed as Folate receptor alpha-high.
This uncertainty-based rejection reveals a key responsibility of NICE – confidence in the therapies put forward by pharma. When a pharmaceutical company puts forward their therapy without sufficient evidence to support their claim, NICE cannot approve the drug as a method of protecting the system from spending on a therapy which may not provide a real-world benefit. The trade off? Leaving patients without a life-saving drug.
Case study 3: Avastin® in combination with platinum-based chemotherapy for metastatic ovarian cancer.
Avastin® (Roche) is an anti-angiogenic therapy which blocks the formation of new blood vessels essential for tumour growth. Avastin® in combination with platinum chemotherapy is FDA and SMC approved for multiple indications of platinum-resistant recurring ovarian, fallopian tube and peritoneal cancers.
In 2019, NICE were unable to provide guidance on the use of Avastin® with platinum chemotherapy due to Roche failing to provide evidence submission. Whilst published data shows significantly improved progression-free survival and platinum sensitivity recurrence, the lack of sufficient evidence being provided for NICE assessment, restricted their ability to approve the therapy for NHS usage. There are 5,000 new cases of metastatic ovarian cancer in the UK, annually.
Roche’s decision not to provide an evidence submission reveals a gap in the drug appraisal system – NICE can only evaluate based on information they’re given. The lack of, by pharmaceutical companies, could be for a range of reasons but ultimately means UK patients lose access before a formal assessment can be made. A business decision made without considering clinical need.
The hidden cost of rejection
NICE decisions consider taxpayers money, which funds the NHS and the services it provides. When therapies are rejected, the trade-off is protecting NHS budgets but potentially restricting patient access to vital treatment, deepening health inequalities and delaying future pharmaceutical innovation.
Even within the NHS, access to rejected drugs is inconsistent. Some become available through the Cancer Drugs Fund or due to an individual NHS trust’s decision to deliver the drug, creating a postcode lottery where the same diagnosis receives different regimes depending on geography. There is a lack of transparent criteria for which trust funds which drug and the process can take some time with special approval.
Rejected drugs are sometimes available through private pathways at a significantly higher cost to the patient – costs vary on the treatment and cancer type but often start from £2K per cycle. Some patients travel internationally for treatment (a phenomenon termed medical tourism) when a drug is rejected by NICE and NHS use. Both options create a two-tier system in which wealthy patients access cutting-edge treatments whilst NHS patients do not, worsening the existing survival disparities by income and deprivation.
What the threshold changes don’t solve
The April 2026 threshold increase from £20K – £30K to £25K – £35K per QALY should theoretically allow more cancer drugs being approved based on cost-benefit analysis; NICE anticipate an approval of 3-5 more drugs per year overall. Whilst this sounds positive, the NHS budget is largely fixed and already overstretched. Every pound used to approve a new cancer drug, is a pound unavailable elsewhere. What gets deprioritised? Prevention measures, mental health or social care resources – who decides which of these becomes less valuable to make room for a new cancer drug? The trade-off is real but rarely made explicit.
The threshold changes don’t address the root cause – drug pricing. Pharmaceutical companies set prices they know many markets will pay regardless of cost-effectiveness. The UK has a weaker negotiating power than larger markets like the US or EU, and the new threshold changes reward higher pricing strategies rather than challenge them. The system adapts to expensive drugs rather than demanding they become more affordable.
Then comes the inequality implications. Higher thresholds for cancer drugs may be justifiable based on severity, but what about those with less “sympathetic” conditions? With finite resources mental health, chronic pain management and preventative care are more likely to be deprioritised. The policy choice then becomes: prioritise life-extension in late stage cancer vs invest in prevention measures that prevent the cancer from arising in the first place.
Every NICE threshold increase, every drug approval, every rejection reshapes who gets treatment and who doesn’t. The current system is designed to make rational economic decisions, but those decisions have significant human consequences that fall unevenly across income, geography and disease type.
The QALY framework gives NICE a rational way to make impossible decisions but with deeply unequal outcomes – rejections are painful for patients and unequal in their impact. Wealthier patients access rejected drugs privately, geography dictates NHS treatment regimes and every threshold increase that approves more cancer therapies, deprioritises something else just as important. The system is working exactly as designed, but does it reflect the healthcare system we actually want?

Leave a comment